Will AI Replace Speech Therapists? A Texas SLP's Honest Answer
The question comes up more than you might expect.
Parents ask it when they find an app that promises to fix their child's R sound without a therapist. SLPs ask it when they wonder what their profession will look like in ten years. And the companies building AI speech tools are happy to let the question sit unanswered — because uncertainty is good for business.
So here is my honest answer, from someone who has spent years in this field and built a virtual practice specifically because I believe technology — used correctly — can help more children get better care.
No. AI will not replace speech therapists. But the conversation is worth having — because understanding why tells you a great deal about what good speech therapy actually is, and why access to it is more complicated than most people realize.
The SLP Shortage Is Real — And Getting Worse
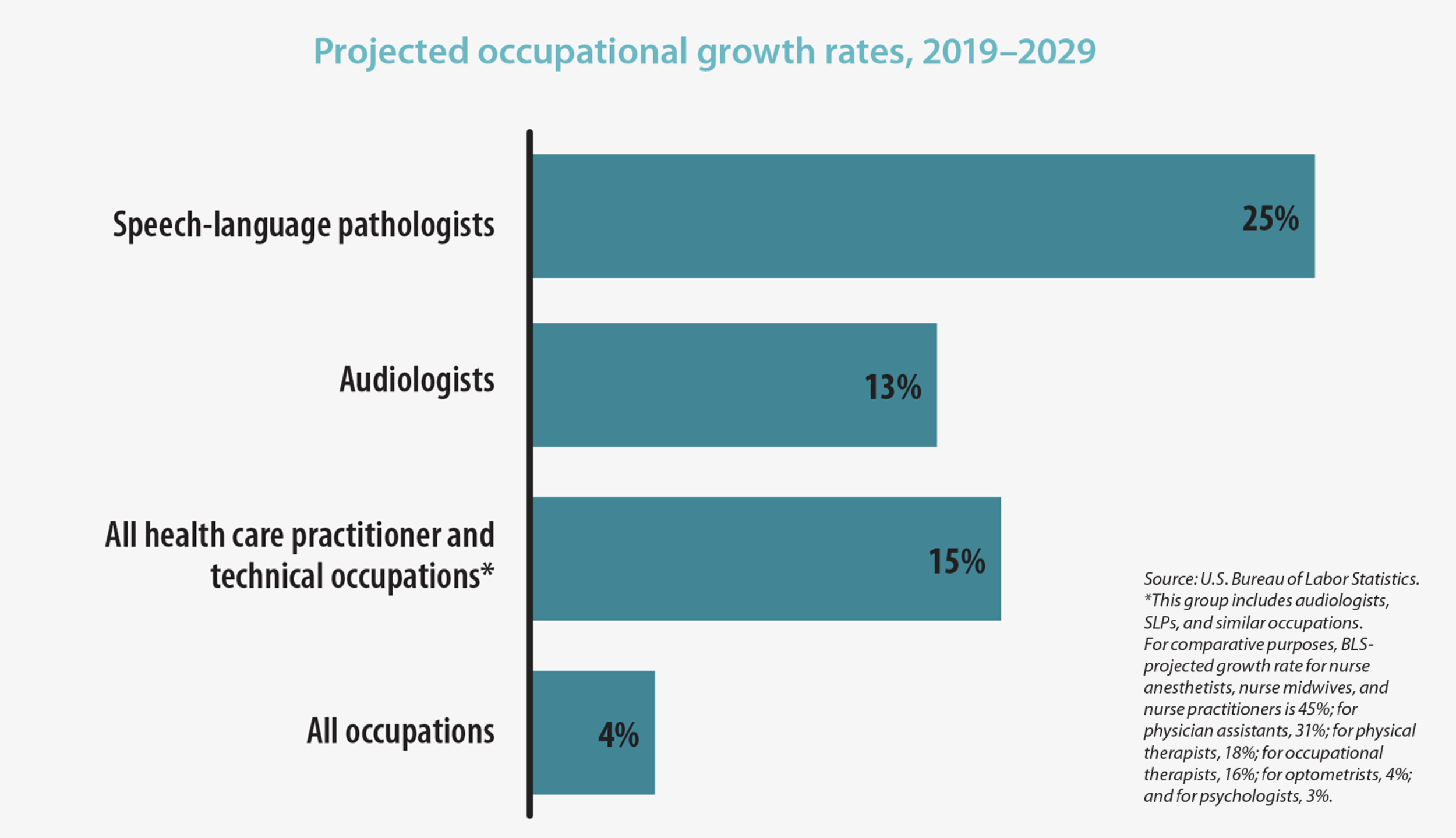
The speech-language pathology profession is projected to grow 25% over the 2019–2029 decade, considerably greater than the average (4%) for all occupations, according to the Bureau of Labor Statistics (BLS).
Before we talk about AI, we need to talk about the problem it is supposedly solving.
There is a genuine, documented, and growing shortage of speech-language pathologists across the United States. ASHA has identified critical shortages in all regions of the country, particularly in school settings. According to the Bureau of Labor Statistics, employment of SLPs is projected to grow 15% from 2024 to 2034 — far faster than the average for all occupations — with about 13,300 new openings projected each year over the decade.
The profession cannot keep up.
In 2024, 78.5% of school-based SLPs reported that job openings in their area exceeded the number of available candidates. Nearly half of funded SLP positions in healthcare settings remain unfilled. Graduate programs are limited in capacity. Experienced clinicians are retiring faster than new ones are entering the field. And the children who need services — more of them every year, as autism rates rise, awareness grows, and early identification improves — are waiting.
In schools, this means children on waitlists, caseloads that are unmanageable, and SLPs stretched so thin that meaningful specialist-level care becomes nearly impossible regardless of skill.
In private practice, it means families driving long distances to find a qualified provider, paying out of pocket because insurance doesn't always cover speech therapy, and waiting months for an evaluation even when they can afford one.
I hear from SLPs regularly — from across the country — asking how I built CloudSpeech, whether they can start a virtual practice, how they can continue doing meaningful work without driving between schools or paying the overhead of a physical clinic. These are not people leaving the field. They are people trying to stay in it on terms that are sustainable.
And they are not alone. A clinic I came across in California has grown so rapidly that over 80% of their team now delivers services virtually — not because they planned it that way, but because they could not hire fast enough any other way. They still have a waitlist.
This is the landscape into which AI speech therapy apps have arrived.
What AI Can and Cannot Do
Let me be clear about what the current generation of AI speech apps actually offers.
Most use machine learning to detect speech errors and provide automated feedback. A child speaks into a device, an algorithm analyzes the production, and the app responds. In narrow, specific contexts — particularly older children or adults drilling a single familiar sound — there is early research suggesting these tools can support practice.
Support. Not treatment.
A 2025 review published in ASHA's own journal found that AI clinical speech tools have generally not yet lived up to their potential, particularly for children. Three consistent problems remain: not enough training data from children's voices, meaningful bias by age and gender, and very limited high-quality evidence showing real clinical outcomes in real children.
What AI cannot do is diagnose. It cannot tell the difference between a frontal lisp and a lateral lisp — two conditions that require entirely different treatment approaches. It cannot recognize Childhood Apraxia of Speech. It cannot adapt when something isn't working. It cannot notice that a child is shutting down and pivot to something different before the session falls apart. And it cannot build the therapeutic relationship that makes a child willing to try the hard thing one more time.
An app is a tool. A speech therapist is a clinician.
Teletherapy Is Not an App
This is the distinction I find myself making most often — and it matters more than most parents realize.
Teletherapy is real therapy, delivered by a real licensed clinician, through a screen. One person. One child. Evidence-based treatment. Clinical judgment in real time.
An AI app is automated feedback delivered by an algorithm with no clinical training, no diagnostic capability, and no ability to adapt to what it sees in front of it.
These are not the same thing. They are not even close.
Teletherapy works because the clinician works. The screen is just the medium. The relationship, the expertise, the real-time adaptation — that is what produces outcomes. And the research supports it: multiple systematic reviews confirm that teletherapy delivers comparable or better outcomes than in-person therapy for most speech and language disorders in school-age children.
What teletherapy also does — and this is why I believe in it so deeply — is remove the access barriers that are keeping children from getting the specialist care they need.
A family in Midland, Texas should not have to drive three hours to see a CAS specialist. A child in a rural school district with no SLP on staff should not go unserved because the nearest clinic is an hour away. An SLP who wants to serve families well but cannot sustain the overhead of a clinic or the burnout of a school caseload of 80 should not have to choose between their career and their wellbeing.
Teletherapy is not a compromise. For many families, it is the only path to specialist care — and it works.
The Tools Worth Using
I want to be honest about technology playing a genuine role in better outcomes — because some tools are genuinely valuable.
The staRt app, developed by Dr. Tara McAllister at NYU's BITS Lab, is a perfect example. It provides real-time acoustic biofeedback during R sound therapy — showing children a visual display of their own speech production so they can see the difference between their error and the target. Research shows children using biofeedback improved 2.4 times faster than those receiving traditional treatment alone.
That is not AI replacing a therapist. That is a clinician using a powerful tool to do something better than they could without it — giving a child information that no amount of verbal instruction can provide on its own.
This is the right model. Technology amplifying clinical skill. Not replacing it.
What Does This Mean for Your Child?
If your child has a speech sound disorder — an R error, a lisp, a phonological pattern, or Childhood Apraxia of Speech — here is what they need:
A qualified, specialist clinician who understands their specific disorder, applies evidence-based treatment, and adapts in real time to what they see.
That clinician might be down the street or they might be in Austin, Texas, serving your family virtually from wherever you are in the state.
What your child does not need is an app making decisions that require clinical judgment — or a waiting list that stretches months because the system cannot keep up with demand.
Speech therapy is still a young profession. It has been undervalued, underfunded, and understaffed for years. The shortage is real. The need is growing. And the solution is not an algorithm.
The solution is more qualified clinicians with better tools, better access models, and the freedom to do their best work — wherever that work happens to take place.
That is what teletherapy, done right, can be.
Christina Burnham, MS CCC-SLP Founder, CloudSpeech: Online Therapy cloudspeech.com | 512-765-4554